Content and Layout by Dr Jonathan M. Naylor, Diplomate ACVIM, Dr Anthony P Carr, Diplomate ACVIM, Mr Ryan E. Walker. Funded in part by CONVINCE.
Canine Cardiology
The four basic principles required for successful auscultation are:
- Correct use of the stethoscope.
- Recognition of external landmarks that correspond to valve locations and that due to acoustical effects within the heart, the locations where sounds are heard loudest do not necessarily correspond to their anatomical source.
- Correct differentiation, interpretation and understanding of normal versus abnormal sounds. Studies have shown that both students and veterinary practitioners can correctly describe the physical features of heart sounds, however, their ability to correctly interpret these sounds is often lacking (Naylor et al., In Press). This finding may be because traditional teaching methods rely on a verbal description of an audible anomaly rather than actual audio recordings. The authors of this website hope that with the multimedia technologies used herein, specifically the pairing of actual cardiac audio recordings with visual interpretation, individuals will improve their diagnostic and interpretive skills. For further information on cardiology, you may consult “Hearing Horse Hearts: An Interactive Guide to Equine Cardiac Auscultation” (Naylor, 2000).
- The ability to convey your understanding and interpretation of what you heard to others using standard veterinary terminology.
The Components of a Stethoscope
Most stethoscopes are designed with a bell and a diaphragm. The diaphragm is designed to pick up high frequency sounds and should be held firmly against the skin. The bell is designed to amplify lower frequency sounds when applied with light pressure. When using the bell, avoid applying firm pressure because the skin beneath the bell will act as a diaphragm and negate the amplification of low frequency sounds (Fox, 1988). The ear pieces should fit comfortably in your ear canals. If the stethoscope comes with different sized ear pieces, select the ear pieces that form the tightest seals in your ear canals. The tubing connecting the binaurals to the bell-diaphragm may be single or double layered. Double layered tubing eliminates more background noise.

How To Use a Stethoscope Correctly
For auscultation to be effective, it should be performed in a quiet room with little extraneous noise. The stethoscope is most effective if:
- When placed in the ears, the binaurals follow the same direction as the ear canals (see diagram below).
- The ear pieces fit snugly in the ears forming a tight seal and the hand holding the stethoscope is still, relaxed and placed against the animal with a constant amount of pressure.

Anatomy
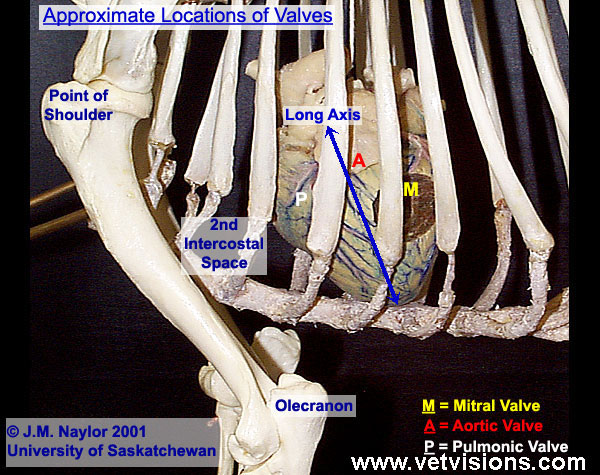
The canine heart projects into both thoracic cavities, particularly the left, from the third to the sixth intercostal space. The long axis of the heart is rotated cranially so that it lies at an angle with the base more cranial than the apex. The base of the heart is fixed by the great veins and arteries while the apex can move freely within the pericardial sac. The so-called right and left sides of the heart are more correctly understood to be the dextrocranial and levo-caudal sides because the left ventricle lies behind and slightly left of the right ventricle. The left ventricle is more conical and massive than the right ventricle which is more crescent shaped.
Landmarks
If the dog is standing square, much of the heart lies medial to the triceps mass. A horizontal line drawn through the point of the shoulder lies slightly above the level of the heart valves. As opposed to using features of the forelimbs (e.g. the point of the shoulder and position of the olecranon) to locate heart valves, palpation of the apex beat is more accurate because its position is independent of the dogs forelimbs.


The Apex Beat
The apex beat is an impact vibration produced at the start of ventricular contraction as the heart hits the chest wall. In the normal dog it is palpated on the left side, ventrally in about the fifth intercostal space. The apex beat should be identified by palpation before the heart is listened to. It is important in lesion localization because the mitral valve lies close by and S1 is loudest at this point.

Cardiac Auscultation
Cardiac auscultation should be performed in a quiet room free of excessive noise. Cardiac auscultation should also be performed as soon as the animal enters the exam room or when the dog is stressed since this increases the probability that a transient or subtle murmur will be detected. The probability of detecting a murmur increases with stress because sympathetic activation increases heart rate, cardiac contractility and cardiac output. Turbulent flow, which gives rise to murmurs, is more likely at higher blood velocities.
Cardiac auscultation should proceed in a logical manner. The apex beat (mitral valve area) should be palpated and the heart rate measured either by cardiac auscultation or palpation of the femoral pulse. The femoral pulses should be palpated in each hindlimb and compared for fullness, sharpness and regularity. Next the femoral pulse should be palpated simultaneously with cardiac auscultation in order to detect pulse deficits due to arrhythmias. Each valve should be ausculted in the order Mitral, Aortic, Pulmonic (acronym MAP). Some palpate the apex beat (mitral valve area) and move cranially from there. However, if you wish to auscult in a particular intercostal space it is easier if you start counting spaces from the last rib (13th) cranially.


Basic Cardiac Function
The cardiac cycle consists of two phases: Systole (ventricular contraction) and diastole (ventricular relaxation). At rest, systole occupies one-third of the cardiac cycle while diastole occupies two-thirds of the cardiac cycle. The normal rhythm (Poodle example below) originates from the sino-atrial node. When the rhythm is completely regular (the timing of the heart sounds remain in a uniform, repeating cycle) it is called a normal rhythm. Sinus rhythm refers to the normal rhythmic contractions of the heart initiated after the sino-atrial node discharges. It may be completely regular or the interval between beats may wax and wane. This is referred to as sinus arrhythmia and is normal in dogs. An ECG (electrocardiogram) is required to confirm the presence of sinus rhythms or arrhythmias. In the following table the width of the columns represent the duration of the audible characteristics of the cardiac cycle. All of the normal characteristics of the cardiac cycle are represented in this Normal Cardiac Cycle Characteristics movie below.

Audible Sounds Detected During Auscultation
Research has revealed that there are four main sounds produced during the cardiac cycle of which only the first and second are normally heard in canines. The third and fourth heart sounds are pathological if ausculted.
Normal
S1 – The first heart sound (lub) is the result of the closure of the left and right atrioventricular valves (mitral or bicuspid and tricuspid valves respectively).
S2 – The second heart sound (dup) is the result of the closure of the pulmonic and aortic (semilunar) valves.
Pathological
S3 – The third heart sound is the result of the addition of more blood into a partially filled ventricle thus creating turbulence and sound waves.
S4 – The fourth heart sound is the result of atrial contraction. Although S4 is labelled the fourth heart sound; if present; it will be heard at the start of the cardiac contraction cycle.
The First and Second Heart Sounds
Listen to the recordings below of isolated heart sounds and see if you can detect the differences in duration, intensity and pitch. S1 is slightly longer in duration and of lower pitch than S2. More reliable clues are the timing of the sounds and that S1 is louder than S2 when you listen at the apex beat.

The Third and Fourth Heart Sounds
In canines, the third and fourth heart sounds (S3 and S4) are not heard in normal animals and their presence is an indication of pathology. The presence of S3 is often associated with dilated cardiomyopathy (DCM) or chronic volume overloads due to acquired mitral insufficiency while S4 is associated with hypertrophic cardiomyopathy, pressure overloads (semilunar valvular stenosis) or chronic hypertension (Fox, 1988). Since S3 and S4 are both low frequency sounds, they are best heard with the stethoscope bell.

Other Normal Sounds
Other normal sounds include those sounds produced by the gastrointestinal tract and the respiratory tract. Both gut and respiratory sounds are clearly distinguishable from cardiac sounds. The gut sounds will be variable and irregular in timing while the respiratory sounds are consistent and regular in timing.

Artifacts
During cardiac auscultation you can hear additional sounds produced by movement or the environment. In order to eliminate these sounds the location where auscultation is being performed should be free of excessive noise, the dog should be properly restrained and the vet should take care in handling the stethoscope. To reduce the sound of hair rubbing (audio sample below) against the stethoscope, the dogs coat may be moistened with alcohol over the target area.

Normal Resting Heart Rate Values for Canines
The “normal” heart rate for canines varies with the age, physical size, breed, level of arousal and physical condition of the animal (Tilley and Goodwin, 2001). Smaller dogs have faster heart rates than larger ones. Compare the recordings from an adult Poodle with that from a Greyhound (both audio samples below), and use your watch to practice taking the heart rate. As a general rule, clinicians will take the heart rate over a period of 10 or 15 seconds depending on how tachycardic the animal is. If you have difficulty counting the faster rate try counting in tens and remembering every set of ten by extending a finger. The answers can be found by hovering over here.Poodle = 102 bpm; Greyhound = 78 bpm

Arrhythmias
An arrhythmia or dysrhythmia is a deviation from the regular rhythm. In dogs this may be normal or abnormal and may result from abnormal cardiac impulse formation, conduction, rate or regularity.
Regularity
Regularity refers to the predictability of an arrhythmia. Some arrhythmias occur in a predictable fashion and are said to be regularly irregular. These rhythms may be normal (e.g. sinus arrhythmia) or pathological. In others the onset of the next beat is completely unpredictable and the rhythm is said to be irregularly irregular (e.g. atrial fibrillation). Irregularly irregular rhythms are pathological in origin.
Classification of Arrhythmias
Tilley and Goodwin (2001) classify arrhythmias according to:
Origin – Supraventricular arrhythmias arise from the atria or AV node whereas ventricular arrhythmias arise from the ventricles.
Rate – Arrhythmias with slow rates are bradyarrhythmias while those with fast rates are tachyarrhythmias.
Regularity – Fibrillation is a rapid, irregular, chaotic rhythm while tachycardia is a rapid but regular rhythm.
Normal Sinus Impulse Formation
Sinus arrhythmia is a regularly irregular sinus rhythm which is a normal finding in most dogs (especially brachycephalic breeds). Sinus Arrhythmia is characterized by slight variations in the S1-S1 interval. These variations are related to changes in vagal tone to the heart and are often associated with inspiration (negative pressure created in the thorax) or use of sedative or anesthetic drugs. You can demonstrate sinus arrhythmia by palpating the radial artery on your wrist. Once you feel your pulse take a big deep breath and you should feel your pulse quicken and then slow down as you exhale.
Altered Sinus Impulse Formation
Sinus Bradycardia (Slow Heart Rate)
Sinus bradycardia has a regular rhythm and may result from systemic disease (renal failure), toxicities, increased vagal tone, elevated intracranial pressure or compression of the eyeball, hypothermia, hypothyroidism or drugs (tranquilizers, propranolol, morphine, various anesthetics) (Fox, 1988). Sinus bradycardia is diagnosed when the heart rate is less than 65 beats / minute and an ECG shows sinus rhythm.
Sinus Tachycardia (Increased Heart Rate)
Sinus tachycardia; often caused by stress; is the most common arrhythmia observed in dogs and has a regular rhythm. Sinus tachycardia may result if there is increased metabolism and oxygen demand or increased requirement for cardiac output (pain, fright, excitement), pathology (fever, shock, anemia, hypoxia, hyperthyroidism) or pharmacological agents (atropine, epinephrine, ketamine) (Fox, 1988). Sinus tachycardia is diagnosed when the heart rate is greater than 160 beats / minute for most dogs (>180 bpm for small / toy breeds or >220 bpm in puppies) and an ECG shows sinus rhythm (Fox, 1988) .
Altered Supraventricular Impulse Formation
Atrial Fibrillation
Atrial fibrillationFibrillation refers to the situation in which muscle tissue spontaneously enters a state of rapid, irregular and completely random contractions. is a common pathological arrhythmia in dogs (atrial fibrillation example shown below). Auscultable characteristics of atrial fibrillation include a completely unpredictable rhythm, sometimes called a “jungle drums” rhythm. Listen for long diastolic pauses between some beats and very short intervals between others. Sometimes the beats are so close together that S2 is not generated and two S1 sounds follow each other. The other hallmark of atrial fibrillation is a pulse deficit. Sometimes this can be detected because there is a large disparity between the heart rate and the pulse rate. If the heart beat is slow it is more reliably detected by simultaneous auscultation and palpation of the pulse. Normally every S1 heart sound is followed by a pulse wave. Abscence of a wave is called a pulse deficit.
The most common causes of atrial fibrillation are chronic atrioventricular valvular insufficiency in small breeds, dilated cardiomyopathy in large breeds, and congenital heart defects. Less common causes include heart worm disease, cardiac trauma, digitalis toxicity and severe metabolic disorders (Fox, 1988). Auscultable or palpable characteristics of atrial fibrillation include inconsistently filled femoral pulses, detection of an S1 without an S2 and a pulse deficit.
Disrupted Impulse Conduction
Second Degree Atrioventricular (AV) Block
Second degree AV block may be of two types: Mobitz I, usually type A or Mobitz II, usually type B. The two types of second degree AV block are best distinguished by ECG. Mobitz I is a normal finding in dogs, especially in young animals and disappears with exercise. Mobitz II is pathological in origin and will not disappear with exercise. Both types of second degree AV block are manifested by a dropped beat detectable during auscultation.
By exercising and immediately ausculting the dog, you can determine if the AV block is a Mobitz I (the dropped beats have disappeared) or Mobitz II (the dropped beats are still auscultable). Second degree AV blocks can be associated with sinus arrhythmia, increased vagal tone, supraventricular tachycardia, electrolyte imbalances or drugs (digitalis, intravenous atropine, xylazine) (Fox, 1988).
Murmurs
Murmurs are sounds produced by turbulent blood flow. Rapid flow, a wide vessel, low blood viscosity and an uneven or constricted vessel wall all predispose to cardiac murmurs. They can be physiological, for example high blood flow though the aortic outflow tract. Pathological murmurs reflect heart disease, for example degeneration and roughening of a valve surface. Veterinarians require a uniform method of describing murmurs to facilitate communication between each other via a common understanding. Five parameters have been developed that serve to describe all of the important aspects of a murmur. Of the five parameters, the most important ones are position in the cardiac cycle, intensity, duration and pattern of intensity. The point of maximal intensity (PMI) identifies the location where the murmur is heard loudest and is often described using the valve location nearest (e.g. Mitral valve area). A table below summarizing the parameters and their descriptions (Naylor, 2000). In dogs, systolic or continuousContinuous murmurs occur throughout both systole and diastole and are associated with patent ductus arteriosus (PDA). murmurs are more common than diastolic murmurs (diastolic murmur example).
In describing the duration of murmurs, panPan describes the duration of murmurs which last from the beginning of S1 to the end of S2 or the beginning of S2 to the end of S1 and thus the murmur obliterates both of these heart sounds. refers to a murmur that obliterates both heart sounds either through systole or diastole but does not obliterate any heart sounds. HoloHolo describes the duration of murmurs which last from the end of S1 to the beginning of S2 or the end of S2 to the beginning of S1 and these murmurs do not obliterate S1 or S2. refers to a murmur that lasts throughout stystole or diastole but does not obliterate any heart sounds. A continuous or machineryMachinery describes a murmur that occupies most of systole and diastole and may be used interchangeably with continuous. murmur (PDA video example below) lasts throughout most or all of systole and diastole and may or may not obliterate heart sounds. Early- and late describe murmurs that are positioned closer to one heart sound than to another. Crescendo, decrescendo or diamond are terms that describe the intensity profiles of murmurs as increasing, decreasing or increasing and then decreasing in loudness. MusicalMusical describes the frequency profile of a murmur where there is a single prominent primary or fundamental frequency with secondary harmonics. and blowingBlowing describes the frequency profile of a murmur in which there is no single predominant frequency.
and blowingBlowing describes the frequency profile of a murmur in which there is no single predominant frequency. are terms used to describe the frequency profile of a murmur. Grade refers to the absolute intensity of murmurs determined on a 6 point scale where the higher the grade the more severe the murmur (Example: Grade 2 versus a grade 5 regurgitant murmur).
are terms used to describe the frequency profile of a murmur. Grade refers to the absolute intensity of murmurs determined on a 6 point scale where the higher the grade the more severe the murmur (Example: Grade 2 versus a grade 5 regurgitant murmur).

Research shows that most clinicians correctly describe the grade of a murmur. Localization of the murmur to systole or diastole is less consistent. A clue is the timing of the heart sounds (systolic murmurs occur in the short pause), however loud murmurs can be perceived as being of longer duration than they really are (Naylor et al., In Press). Another useful method is to palpate the pulse during auscultation. Pan- or holo-systolic murmurs should be heard coincident with the pulse wave.
Problems and Strategies for Murmur Localization
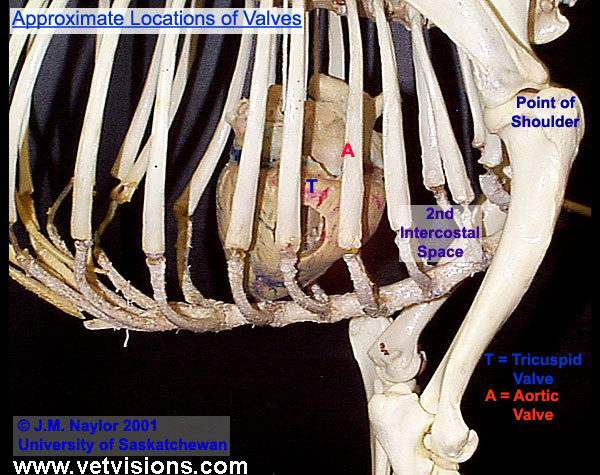
On the left side, the pulmonic and aortic roots lie next to each other and it is difficult to separate their respective valvular sounds. Both produce sounds that are best heard cranio-dorsally on the left side of the thorax at the second or third intercostal spaces. Since the aortic valve is more centrally located and produces louder sounds some aortic murmurs are also heard on the right side. Mitral valve problems produce sounds that are heard more caudally centered on the fourth or fifth intercostal space. On the right side, tricuspid and ventricular septal defects produce murmurs that are heard ventrally around the fourth or fifth intercostal space. A problem with localizing the origin of murmurs is that loud murmurs can radiate over a wide area and on both sides of the thorax. Despite this, the point at which they are loudest is often close to the lesion.
Sometimes it may prove challenging to correctly identify the likely origin of a murmur. Generally by following a logical process like the one outlined here, insight may be gained into the type of murmur being dealt with. First of all the stethoscope should be moved around to all the valve areas on each side of the thorax in order to ascertain where the PMI is located and which; if any; valve is involved. With the location of the PMI known the murmur’s intensity may be accurately graded and the character and quality judged. Finally, by simultaneously ausculting the PMI and palpating the femoral pulse an accurate indication of the position and duration of the murmur within the cardiac cycle may be obtained. Additionally, note that by examining the animal as soon as it enters the exam room or when it is stressed, the probability of detecting a transient or subtle murmur increases because the intensity increases in accordance with the sympathetic effects of stress.
The Most Common Murmurs Afflicting Dogs and their Features
In order of prevalence:
Mitral Regurgitation
Mitral Reguritation, the result of mitral insufficiencyInsufficiency when related to any one of the four heart valves refers to the situation in which the valve fails to close properly. Blood flows against its normal course producing turbulence and a murmur., allows backflow of blood into the left atrium. Typical features of mitral regurgitation include a normal to increased arterial pulse, a PMI located at the left apex, a plateau or decrescendo quality and systolic position in the cardiac cycle (example below) (Fox, 1988). Mitral regurgitation is most often the result of acquired valvular disease (e.g. mitral valve endocardiosis) and is usually observed in older dogs.
Patent Ductus Arteriosus
Patent ductus arteriosusPDA is a congenital condition characterized by the post-natal persistence of a lumen in the ductus arteriosus between the aorta and the pulmonary artery. PDA is manifested by a continuous murmur. (PDA example below) results when the ductus arteriosus fails to close properly (functional closure normally occurs by 72 hours after birth while anatomic closure is complete within the first few weeks). PDA is therefore most commonly seen in young dogs with a higher prevalence in purebreds and females (Fox, 1988). This murmur will feature an increased arterial pulse, a normal to increased venous pulse, a PMI located at the left base and a machinery or continuous quality as it is present throughout most or all of systole and diastole (Fox, 1988).
Tricuspid Regurgitation
Tricuspid regurgitation, the result of tricuspid insufficiency, allows backflow of blood into the right atrium. Like mitral regurgitation, tricuspid regurgitation is most often caused by acquired valvular disease and is usually observed in older animals. Features of a tricuspid regurgitant murmur include an increased venous pulse, a PMI located at the right apex, a plateau or decrescendo quality and a systolic position in the cardiac cycle (Fox, 1988).
The following two diagrams represent the locations where specific cardiac pathologies will be auscultated best.


Terminology
Some of the common terms used in cardiology are:
- Blowing describes the frequency profile of a murmur in which there is no single predominant frequency.
- Continuous murmurs occur throughout both systole and diastole and are associated with patent ductus arteriosus (PDA).
- Crescendo describes an intensity pattern of a murmur that increases as it progresses towards completion.
- Crescendo-Decrescendo – See Diamond-Shaped
- Decrescendo describes an intensity pattern of a murmur that decreases as it progresses towards completion.
- Diamond-Shaped refers to an intensity pattern of a murmur that first increases and then decreases towards completion.
- Fibrillation refers to the situation in which muscle tissue spontaneously enters a state of rapid, irregular and completely random contractions.
- Flutter describes a state of rapid, regular and uniform muscular pulsations or contractions in the range of 200-320 per minute.
- Holo describes the duration of murmurs which last from the end of S1 to the beginning of S2 or the end of S2 to the beginning of S1 and these murmurs do not obliterate S1 or S2.
- Insufficiency when related to any one of the four heart valves refers to the situation in which the valve fails to close properly. Blood flows against its normal course producing turbulence and a murmur.
- Machinery describes a murmur that occupies most of systole and diastole and may be used interchangeably with continuous.
- Musical describes the frequency profile of a murmur when there is a single prominent primary or fundamental frequency with secondary harmonics.
- Pan describes the duration of murmurs which last from the beginning of S1 to the end of S2 or the beginning of S2 to the end of S1 and thus the murmur obliterates both of these heart sounds.
- PDA (Patent Ductus Arteriosus) is a congenital condition characterized by the post-natal persistence of a lumen in the ductus arteriosus between the aorta and the pulmonary artery. PDA is manifested by a continuous murmur.
- Plateau describes an intensity pattern of a murmur that remains constant through to completion.
- Stenosis when related to any one of the heart valves, chambers or great vessels refers to the situation in which the valve fails to open properly or the chamber or vessel is abnormally narrow and the normal flow of blood is hindered.
- Thrill is a vibration caused by turbulent fluid movement through an incompetent valve which is palpable on the thoracic wall. Thrill is typically observed with grade 5 or 6 murmurs.
- Regurgitation results with valvular insufficiency and is characterized by blood flow against its normal course. In canines mitral valve regurgitation is the most common regurgitant-type murmur that will be encountered.
- VSD (Ventricular Septal Defect) is a congenital condition characterized by the persistent patency of the ventricular septum post-natally thus allowing blood to flow directly between the ventricles. Since the blood can bypass the pulmonary circulation cyanosis may be present in addition to a grade 5/6 systolic murmur.
References
- Fox, P.R. 1988. Canine and Feline Cardiology. Churchill Livingstone Inc. New York.
- Naylor, J.M., Yadernuk, L.M., Pharr, J.W. and Ashburner, J.S. In press. An Assessment of the Ability of Diplomates, Practitioners and Students to Describe and Interpret Heart Murmurs and Arrhythmia. Journal of Veterinary Internal Medicine.
- Naylor, J.M. 2000. Hearing Horse Hearts: An Interactive Guide to Equine Cardiac Auscultation. Vet Visions Inc. Saskatoon.
- Tilley, L. P. and Goodwin, J. K. 2001. Manual of Canine and Feline Cardiology 3rd Ed. W.B. Saunders Company. Philadelphia.